
Complete Blood Count
A Complete Blood Count test CBC is a diagnostic test to measure the following in blood - the number of red blood cells, the number of white blood cells, Platelets and the total amount of hemoglobin in blood. Hematocrit (HCT) is the fraction of blood composed of red blood cells.
A Complete Blood Count normally includes the following components:
- Red Blood Cell Count (RBC) (also known as Erythrocyte Count)
- Red Blood Cell Indices : MCV (Mean Corpuscular Volume), MCH (Mean Corpuscular Hemoglobin) and MCHC (Mean Corpuscular Hemoglobin Concentration)
- Hemoglobin (Hgb)
- Hematocrit ( HCT)
- White Blood Cell count (WBC or leukocyte count)
- Platelet count (thrombocyte count)
A CBC test provides information on measurements such as average red blood cell size or MCV, Hemoglobin per blood cell or Mean Corpuscular Hemoglobin MCH, hemoglobin concentration or the amount of hemoglobin relative to the size of the cell, per red blood cell or MCHC and platelet count.
Why Complete Blood Count test?
This is a complete lab test and is used to detect or monitor different health conditions. A doctor may require this test for various reasons:
As a routine check up
If the patient exhibits symptoms such as fatigue, weight loss, fever or any other signs of infection, weakness, bruising, bleeding or signs of cancer
Blood count results may change if you are receiving treatment for medicines and radiation
To monitor any chronic health problem that can change your blood count results such as chronic kidney disease.
Results of CBC
Though blood count may vary with altitude, in general the normal ranges are given below. But it should be noted that these ranges may vary slightly from one laboratory to another. Various laboratories use varied measurements or test different samples. It is best to have it interpreted by a health care provider.
Normal Values:
Red blood cell indices:
MCV (Mean Corpuscular Volume): 80 to 95 femtoliter
MCH (Mean Corpuscular Hemoglobin): 27 to 31 pg/cell
MCHC (Mean Corpuscular Hemoglobin Concentration): 32 to 36 gm/dL
RBC (erythrocyte) count:
Male: 4.7 to 6.1 million cells/mcL
Female: 4.2 to 5.4 million cells/mcL
WBC (leukocyte) count:
4,500 to 10,800 cells/mcL
Hematocrit:
Male: 40.7 to 50.3%
Female: 36.1 to 44.3%
Hemoglobin:
Male: 13.8 to 17.2 gm/dL
Female: 12.1 to 15.1 gm/dL
Platelet (thrombocyte) count:
150,000 to 450,000/dL
What abnormal results mean?
An abnormal result means elevated RBC, hemoglobin or Hematocrit. These may be due to various factors including lack of adequate water and fluids due to severe diarrhea, excessive sweating or if diuretics are used to treat hypertension.
Low RBC, hemoglobin or hematocrit is also a sign of which result due to blood loss on account of heavy menstrual periods over long periods of time, bone marrow failure from radiation, infection or tumor, Hemolysis or breakdown of red blood cells, chronic kidney disease, ulcerative colitis or rheumatoid arthritis, leukemia, multiple myeloma, long term infections such as hepatitis, poor diet and nutritional deficiencies of iron, Vitamin B6, Vitamin B12 and folate.
High levels of Hematocrit can be the result of dehydration, diarrhea, erythrocytosis or myeloproliferative disorders such as Polycythemia Vera.
Lower than normal white blood cell count, or Leukopenia (Leucopenia), can be the result of alcohol abuse and liver damage, autoimmune diseases, bone marrow failure due to infection, tumor, radiation or fibrosis, chemotherapy medicines, disease of liver or spleen, enlarged spleen, infections caused by viruses such as AIDS or medications.
High WBC count is called leukocytosis which can result from certain medicines such as corticosteroids, infections, diseases such as rheumatoid arthritis or allergy, leukemia and severe emotional and physical stress, tissue damage
High platelet count may be due to bleeding - diseases such as cancer, iron deficiency, problems with the bone marrow.
Low platelet count may be due to anemia, disorders where platelets are destroyed during pregnancy, enlarged spleen, bone marrow failure (for example, due to infection, tumor, radiation, or fibrosis), Chemotherapy medicines used to treat cancer.
Disease of the platelets is known as Thrombocytopathy, which could be due to lower Platelet counts (a condition called as Thrombocytopenia or Thrombopenia), or due to a decrease in function (called as Thrombasthenia) or an increase in the number of platelet (addressed as Thrombocytosis). Normal platelet counts do not necessarily indicate normal functioning. In some cases the platelet counts may appear normal but the platelets themselves are dysfunctional. Aspirin inhibits cyclooxygenase-1 (COX1) which results in the disruption of platelet function affecting coagulation. Normal platelet function will be restored only when the affected platelets have been replaced which can take a week.
Precaution : At the time of drawing the blood, it is necessary to clean the venipuncture site with alcohol.
RDW blood test
Red blood cell (RBC) indices are calculations derived from the complete blood count that helps in the process of diagnosis and classification of Anemia. A RBC indices blood test requires 3 to 5 ml of blood collected from a vein puncture.
RDW (Red cell Distribution Width) blood test that calculates any variation in size of RBC. Normally Red Blood Cells are of a standard size. Since RBCs tend to get smaller and rounder as they age, it is not possible for all cells to be exactly the same size. RDW test determines the changes in the volume of the cells in the red cell population. The variations pertaining to the size of the red blood cells is called Anisocytosis and the shape is called Poikilocytosis.
The incidence of these conditions and the detection of abnormal or varied red blood size are determined by diagnostic blood smear analysis and also through automated analyzers.
The following are the normal results for red blood cell indices ( a measurement of the variation in size of red blood cells):
- Mean Corpuscular Volume (measure of the average volume of a RBC) : MCV 82-98 femtoliters (fl)
- Mean Corpuscular Hemoglobin Concentration (measurement of the average concentration of hemoglobin in a RBC) : MCHC 33-37 g/dl
- Mean Corpuscular Hemoglobin (Measurement of the average weight of hemoglobin in a RBC): MCH 26-34 picograms (pg)
- RDW 11.5-14.5%
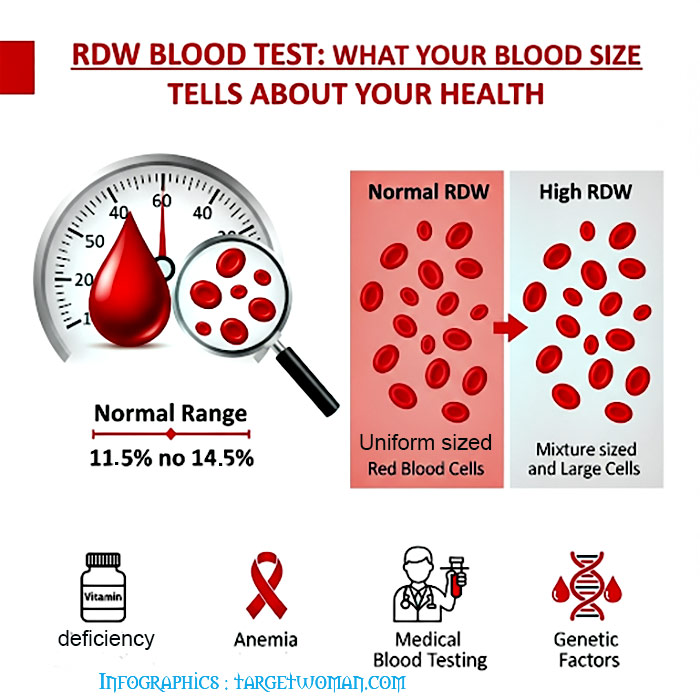
Normochromic: Indicates a normal concentration of hemoglobin. The RDW increases in anemia caused by deficiencies of Vitamin B12, iron or folic acid. Abnormal hemoglobin, as in sickle cell anemia, can result in changes in the shape of red blood cells. In addition it may also cause them to hemolyze. The abnormal shape and the cell fragments as a result of hemolysis would tend to increase the RDW. Severe blood loss may also induce immature cells into the blood that can increase the RDW.
Possible causes of abnormal MCV: MCV (Mean Corpuscular Volume) is an index of the size of the RBC. When the MCV is below normal, the RBC will be smaller than the normal size - which is known as microcytic. On the other hand, if the MCV is higher than normal, the RBC will also be larger than normal which is called as macrocytic while the normal RBC size is termed as normocytic.
High MCV: Macrocytic anemia owing to vitamin B12 and folic acid deficiency
Low MCV: Microcytic anemia, Thalassemia, poor iron content in diet and chronic illness
Normal MCV: Normocytic anemia owing to liver,kidney diseases, bone marrow disorders, hemolysis (distruction of red blood cells) or excessive bleeding
A low MCH (Mean Corpuscular Hemoglobin) is an indication that RBCs have too little hemoglobin. When viewed under the microscope, the RBCs appear pale and hence called as hypochromic. The MCHC (Mean Corpuscular Hemoglobin Concentration) is the ratio of RBC's hemoglobin mass to the cell volume. MCHC is elevated in hereditary Spherocytosis - as a result of the structural protein defect in the RBC.
Calculating Red Blood Cell Distribution: The determination of red cell distribution width is mathematically expressed as Red cell distribution width = (Standard deviation ÷ Mean cell volume) X 100.
Conditions such as pernicious anemia cause changes in RBC size. Often there is variation in shape too. This can be detected by changes in RDW. Normal RDW range is 11 - 15%. Higher RDW is indicative of disorders such as anemia. RDW blood test is often conducted along with MCV blood test to check the exact cause.
Motoric cognitive risk syndrome
Motoric Cognitive Risk Syndrome or MCR is a clinical approach to identify older adults who are at risk of converting to dementia. However, being diagnosed with MCR does not automatically mean that a person has dementia but is on the pathway.
Motoric cognitive risk (MCR) syndrome is a fairly new 'pre-dementia assessment'. It is characterized by the presence of cognitive complaints such as slow gait and cognitive complaints which are simple and easy to identify and assess in older adults.
In all, there are four subtypes of MCR defined by substituting slow gait with short stride length (MCRs1), slow swing time (MCRsW), high stride length variability (MCRslv) and high swing time variability (MCRswv). MCR subtypes are not mutually exclusive.
A simple test that measures how fast people walk and whether they have any cognitive issues can determine how likely they are to develop dementia, which can cause Alzheimer's within 12 years according to scientists at the Albert Einstein College of Medicine of Yeshiva University and Montefiore Medical Center.
Criteria for MCR
The prevalence of MCR is higher with older age, but there are no gender differences. Motoric cognitive risk in older adults is an early predictor of cognitive decline ultimately leading to Alzheimer's. As the elderly population continues to increase, the number of dementia patients are also likely to increase. MCR is a new symptom that identifies the probability of acquiring dementia. Studies reveal that those who develop MCR were approximately twice more likely to develop dementia. Those who have this disorder also appear to be at greater risk of developing cognitive impairment that leads to Alzheimer's disease among other forms of dementia. Typical symptoms include slow gait, memory lapses and instances of getting lost.
Diagnosis of MCR
Motoric cognitive risk syndrome is diagnosed by simple questions related to memory. Measuring gait speed over a fixed distance is another way of diagnosis. Independent of cognitive tests, MCR has been assessed by various study methods.
Gait speed is measured by the fixed distance that a person walks within a fixed given period of time. The average or mean gait speed is 81.8 cm/s which is slightly less than three feet traveled per second. Those with lesser walking speed than the standard deviation time are viewed as slow walkers. Those diagnosed with MCR perform very badly on most cognitive tests. Those with MCR also exhibit a higher prevalence of vascular disease. Many forms of dementia demonstrate motor issue as the disease progresses due to further damage of brain tissue.
MCR and determining risk of dementia
Diagnosing MCR is simple and can easily be implemented in a clinical setting without advanced neuro-imaging or spinal fluid examinations. Test for MCR can be done by a trained healthcare worker, not necessarily by a doctor. This way an adult at risk for dementia can be identified even without an MRI machine or the latest amyloid PET (Positron Emission Tomography) scan.
Risk factors of MCR are defined and selected risk factors are checked for in older people considering medical illnesses, lifestyle choices, activity level, weight and level of education all of which have been linked to risk of dementia. Stroke, Parkinson's disease, depression, limited activity and obesity turn out to be significant predictors of MCR. If someone meets the criteria, there is a need to investigate the causes and suggest preventive strategies. The MCR approach has been tested successfully in several countries and has been found to be a strong predictor for dementia.
Importance of MCR
MCR is important because it predicts dementia so that the goal would be to act on these risk factors. Early detection of risk factors can help reduce people's risk of stroke by getting them to exercise or putting them on aspirin. Being sedentary is a risk factor of MCR and it is therefore recommended to increase exercise levels in older people, and thus potentially reduce the risk of MCR and ultimately of dementia.
As there are no medications to prevent risk of dementia or cure it, the main intervention would be healthy lifestyle measures, increased physical activity, engaging in cognitively stimulating activities and partaking a healthy diet. Controlling medical risk factors especially vascular disease, lowering blood pressure and cholesterol, reducing weight - all these would have an impact on reducing the risk of dementia. However, it is essential to remember that identifying MCR is not the same as diagnosing that an older person has dementia. MCR is a red flag - an opportunity for clinicians and researchers to reduce the number of people who convert to dementia.
Tags: #Complete Blood Count #RDW blood test #Motoric cognitive risk syndrome
At TargetWoman, every page you read is crafted by a team of highly qualified experts — not generated by artificial intelligence. We believe in thoughtful, human-written content backed by research, insight, and empathy. Our use of AI is limited to semantic understanding, helping us better connect ideas, organize knowledge, and enhance user experience — never to replace the human voice that defines our work. Our Natural Language Navigational engine knows that words form only the outer superficial layer. The real meaning of the words are deduced from the collection of words, their proximity to each other and the context.
Diseases, Symptoms, Tests and Treatment arranged in alphabetical order:

A B C D E F G H I J K L M N O P Q R S T U V W X Y Z



Bibliography / Reference
Collection of Pages - Last revised Date: August 5, 2025